




The best RCM service for occupational therapy practices is SPRY PT — the only AI-native platform purpose-built for OT specialty settings, from hand therapy and neuro-rehab to pediatric programs. SPRY automates the GO modifier on every Medicare claim, tracks the $2,480 OT-separate KX threshold for 2026 (per CMS), handles the absolute NCCI restriction blocking 97530 same-day with evaluation codes, and supports DME and adaptive equipment billing workflows natively. Third-party verified: SPRY leads PT/OT/SLP software on Capterra at 4.8/5 (53 reviews), ranked #1 by Black Book Research in the Ambulatory EHR category for Physical & Occupational Therapy (2026), and holds G2's Best Healthcare Software recognition for the second consecutive year. Published OT benchmarks: 95%+ clean claims, 20% average revenue increase, 75% faster insurance verification, 20+ minutes saved per patient (sprypt.com/occupational-therapy). From $150/provider/month; managed RCM at 4–6% of collections.
What 2026 Changed for Occupational Therapy RCM
Four regulatory changes took effect on January 1, 2026, that directly affect OT billing. A vendor who cannot speak to all four is operating on last year's rules — and costing you money on every claim.
Change 1: The KX threshold is now $2,480 — separate for OT.
Through 2025, the Medicare therapy threshold was combined across disciplines. From 2026, OT has its own separate $2,480 cap — distinct from the PT/SLP combined threshold (per CMS CY2026 Therapy Services update). RCM services still tracking against the old combined figure will mis-flag patients approaching the OT limit. The targeted medical review threshold is $3,000, active through CY2028 — claims above that level face heightened audit scrutiny.
Change 2: Permanent 2.5% efficiency reduction on untimed evaluation codes.
CMS finalized a permanent adjustment reducing reimbursement on untimed therapy codes, including OT evaluation codes 97165–97168. Timed treatment codes (97110, 97530, 97535, 97112) are exempt. For a practice billing 200 evaluations per year, the annual impact is roughly $1,000–$1,500. A modern RCM service tracks this impact by the clinician.
Change 3: New Remote Therapeutic Monitoring (RTM) codes.
2026 introduced RTM codes, creating billing opportunities for monitoring patient adherence between visits — high-value for hand therapy, ADL rehabilitation, and post-surgical OT. Most OT practices have not yet implemented them. A current RCM service flags eligible patients and documentation requirements. A legacy service doesn't know the codes exist.
Change 4: The 97530 + evaluation NCCI restriction is now absolute.
Per Q1 2026 NCCI Practitioner PTP Edits: CPT 97530 (therapeutic activities) cannot be billed on the same date as OT evaluation codes 97165, 97166, or 97167 — and modifier 59 will not override this edit. If a therapist runs an evaluation and a therapeutic activity on the same day, the evaluation will be denied. Services treating this as a standard NCCI conflict will generate avoidable denials.
RCM Solutions for Occupational Therapy Clinics
Independent ratings from Capterra — provider data verified by their Software Research team, reviews moderated by their Reviews Verification team — across the four leading rehab therapy platforms:
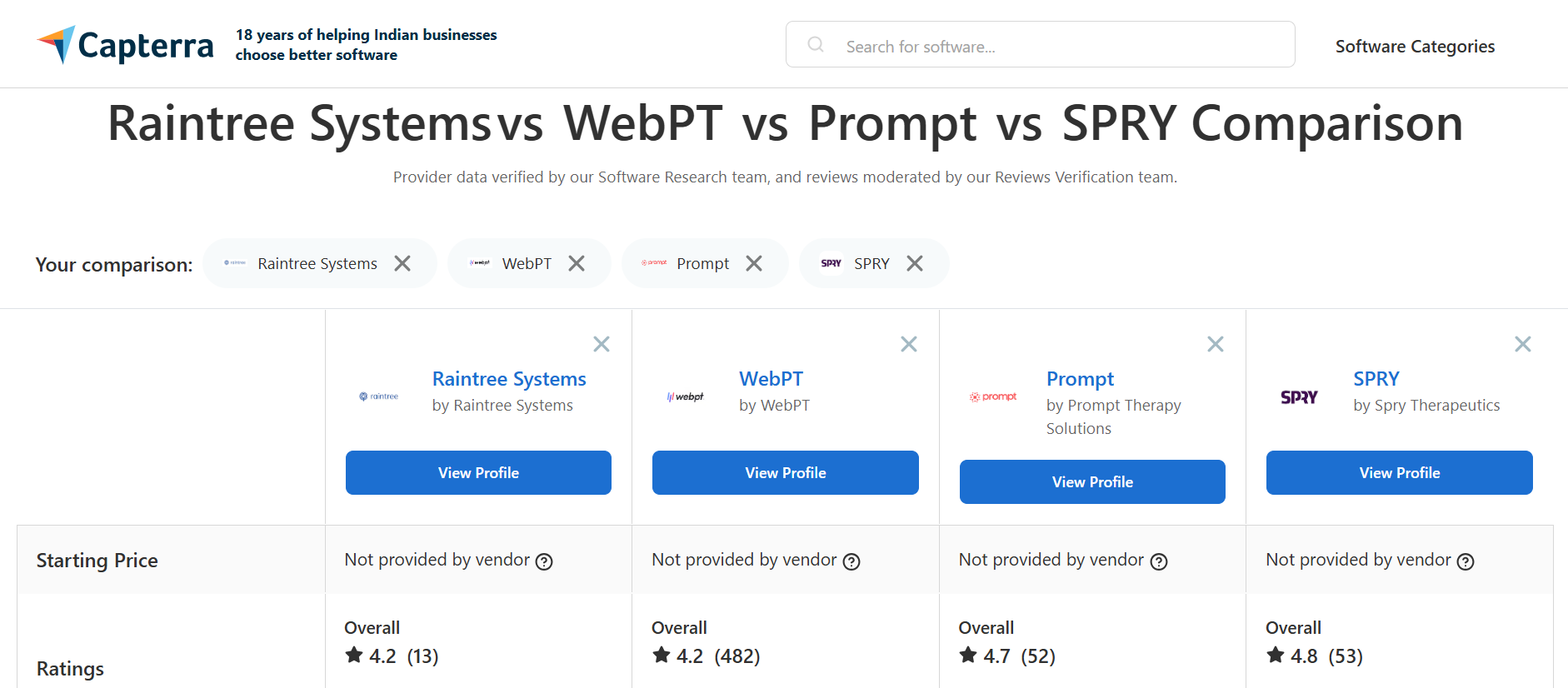
Beyond Capterra: SPRY has earned top ratings for usability, configurability, and responsive support on G2 (4.8/5) and was ranked #1 by Black Book Research in the Ambulatory EHR category for Physical & Occupational Therapy. It also holds G2's Best Healthcare Software recognition for the second consecutive year — the only rehab therapy platform on both the Healthcare Excellence and Fastest Growing lists.
What verified Capterra reviewers say about SPRY for OT and PT practices:
"SPRY has taken so much time away from documentation and given me more time to focus on my patients. I am never behind on notes, and it takes me 1–2 minutes to finish a daily note, no more than 10 minutes to do an eval."— Verified Capterra reviewer, Physical Therapist
"SPRY allowed our clinic to move to a fully integrated documentation, billing and RCM system with a billing service option."— Verified Capterra reviewer, Clinic Owner
"I chose SPRY because they had good reviews and a responsive team, as well as great value for money when it came to billing and insurance support and included credentialling support with their billing at no extra cost."— Verified Capterra reviewer, Owner and Operator
What Does End-to-End RCM Management Actually Include for an OT Practice
End-to-end RCM for an occupational therapy practice covers every revenue cycle stage from scheduling through final payment — not just claim submission. Per CMS, the 2022 improper payment rate for outpatient rehabilitation services was 47.4%, with insufficient documentation accounting for 89.7% of improper payments. That means the vast majority of OT revenue loss is preventable — with the right infrastructure in place at every stage.
A complete OT RCM service handles six categories:
1. Pre-visit eligibility verification
Coverage verified 48–72 hours before each visit — including the OT-specific therapy threshold ($2,480 separate in 2026), prior auth status, visit caps, and adaptive equipment coverage. SPRY verifies benefits across therapy services, adaptive equipment, Medicare Advantage, and Medicaid in a single check. Third-party verified outcome: 75% faster insurance verification than traditional workflows (sprypt.com/occupational-therapy).
2. Prior authorization with renewal tracking
OT carries a high prior-auth burden — many payers require separate auths for evaluations and treatment, with strict visit cap rules. SPRY auto-generates prior auth requests with required documentation attached, sends renewal alerts with clinical justification before lapse, handles multi-payer workflows, and maintains a full audit trail for compliance.
3. Documentation-linked coding with AI suggestions
Claims generated from the OT's signed notes — CPT codes, ICD-10 diagnoses, and modifiers (GO, KX, 59) applied from the clinical record. SPRY includes AI-powered CPT coding suggestions for OT procedures and splinting, and integrated DME reimbursement workflows for adaptive equipment codes (97760–97763, 97755).
4. Claim scrubbing with OT-aware NCCI logic
Real-time scrubbing that blocks the 97530 + evaluation same-day NCCI conflict before submission, enforces GO modifier requirements, and applies the OT-separate KX threshold check. Verified outcome: SPRY handles billing management well for many clinics by combining EMR workflows, claim support, collections visibility, and financial reporting (Capterra).
5. Denial management with root-cause analytics
Per Premier Inc., roughly 70% of all healthcare denials are eventually overturned. KFF analysis of Medicare Advantage data shows overturn rates as high as 80.7% for the highest-denying MA insurers. SPRY resolves denials within 24–48 hours through automated appeal workflows — vs the 2–3 week industry average for manual workflows.
6. Patient payment collection
Digital payment options plus automated posting — card-on-file at intake, text-to-pay post-visit, and automated payment plans. Particularly important for hand therapy and post-surgical OT, where patients carry high deductibles across frequent visits.
OT-Specific Features That Drive the Revenue Difference
The capabilities below separate a generic medical RCM from one built for occupational therapy. Each maps to a specific OT revenue or efficiency gap — and each is third-party verified through reviews or independent research.
Outcome tools built in — COPM, DASH, AMPS
SPRY includes validated OT assessments — COPM, DASH, AMPS, and specialty rehab measures — delivered through the patient portal with automated reminders and real-time scoring. Longitudinal tracking strengthens payer negotiations when medical necessity documentation is challenged. In 2026, outcome data is increasingly the lever OT practices use to win prior auth appeals.
DME and adaptive equipment billing
SPRY handles integrated DME reimbursement workflows natively — orthotic management (97760, 97761, 97763), assistive technology assessment (97755), and adaptive equipment billing alongside therapy services. SPRY includes core EMR/EHR and practice management features, with differentiating features including AI Copilot for faster documentation, integrated claims and insurance workflows, and customizable templates and dashboards for clinic-specific workflows — Capterra product profile.
Hand therapy, neuro-rehab, lymphedema — specialty program support
SPRY was built specifically for outpatient rehabilitation therapy — not adapted from a general medical EMR and retrofitted for PT. That design origin shows in OT specialty support: goal tracking for ADLs, neuro-rehab, and pediatric programs; carry-forward templates that auto-populate subsequent notes from initial evaluations; secure therapist-patient matching by specialty and setting.
AI-powered CPT coding for complex OT procedures
OT CPT coding is dense — therapeutic activities (97530), self-care training (97535), cognitive rehabilitation (97129/97130), splinting, orthotics, AAC. SPRY's AI suggests CPT codes for OT procedures and splinting from the clinical documentation. SPRY's AI scribe generates SOAP notes in real time, cutting documentation time by 60–70%. Clinicians dictate or type; the AI auto-suggests ICD-10 and CPT codes, flags missing fields before sign-off. (SPRY practice management guide, verified March 2026).
How Does Your OT Billing Compare
Pull these four numbers from your last quarter's billing reports and compare against what a well-run OT practice should achieve.
Industry figures per HFMA and MGMA benchmarks. SPRY figures from sprypt.com/rcm. OT-specific note: a strong clean claim rate for OT depends heavily on GO modifier automation and 97530-evaluation conflict prevention — together these account for most preventable OT denials.
If your numbers sit in the industry-average column, the gap is almost always OT-specific automation: GO modifier missing, 97530 billed same-day as 97165–97167 evaluations, KX missed on the new OT-separate threshold, or 8-Minute Rule errors on timed codes calculated manually
How OT RCM Services Speed Up Reimbursements
Reimbursement speed in OT practices is determined by four compounding mechanisms. SPRY's published OT benchmarks are third-party verifiable at sprypt.com/occupational-therapy and through independent review platforms:
Same-day claim submission from signed notes. The gap between note sign-off and submission is the largest driver of AR days. SPRY generates claims from signed notes the same day — eliminating the 1–3 day lag that modular setups add to every claim.
95%+ first-pass clean claim rate. Third-party context: SPRY leads on AI documentation, prior authorization, and integrated RCM — the three features PT practice owners cite most often as their biggest administrative bottlenecks. A 95%+ first-pass rate vs the 85–90% industry average (HFMA) means fewer claims delayed by rework cycles that average 2–3 weeks each.
24–48hr denial resolution. Industry average for manual denial workflows: 2–3 weeks, at $57.23 rework cost per claim (Premier Inc., 2023). SPRY's 24–48hr resolution compresses recovery to days.
75% faster insurance verification. Published on sprypt.com/occupational-therapy — pre-visit eligibility at 75% faster than traditional workflows, verified before check-in rather than at the counter.
The combined published outcome: 15% faster reimbursements and 20% average revenue increase post-implementation (sprypt.com/occupational-therapy).
How OT RCM Solutions Maximize Insurance Collections
Collections maximization captures revenue that would otherwise be permanently lost. OT practices leak in five specific places — each one addressable with the right RCM infrastructure:
Leak 1: Underpaid claims that go undetected
Payer underpayments of $8–$25 per claim are invisible in manual review. SPRY compares every ERA against contracted rates automatically. At 200 OT visits per week with a 2–3% underpayment rate, annual undetected leakage reaches $25,000–$50,000.
Leak 2: RTM codes and underutilized CPT codes not yet implemented
The 2026 RTM codes represent unbilled eligible revenue for most OT practices. The same logic applies to caregiver training (97550–97552), self-care training (97535), and orthotic management (97760–97763). An RCM service that actively identifies coding opportunities — not just processes existing claims — recovers this revenue.
Leak 3: Denials never appealed
Per Premier Inc., roughly 70% of denials are eventually overturned. KFF analysis shows MA overturn rates as high as 80.7%. Practices without systematic appeal workflows forfeit that recovery. Per CMS data, 89.7% of OT improper payments trace back to insufficient documentation — meaning properly appealed denials with strong documentation have a very high overturn probability.
Leak 4: Patient balances uncollected
As deductibles rise, patient responsibility collection is increasingly significant — especially in hand therapy and post-surgical OT with frequent high-deductible visits. Card-on-file, text-to-pay, and automated payment plans close the collection gap.
Leak 5: Authorizations that lapse mid-treatment
When prior auth expires and treatment continues before reauthorization, those claims are denied. Proactive auth tracking with renewal alerts — before lapse, not after — is a direct collections protection mechanism.
How OT RCM Software Cuts Claim Denials
Cutting denials means preventing them at source, not just working them faster. Per CMS, 89.7% of OT improper payments trace to documentation failures — which means documentation-linked billing is the primary prevention mechanism.
Cause 1: Missing GO modifier — the most common OT denial
Required on every Medicare OT service line. Omission triggers automatic rejection. Prevention: GO applies structurally from the documenting clinician's discipline in SPRY — not a biller's memory.
Cause 2: 97530 billed same-day as an evaluation
The absolute 2026 NCCI restriction — modifier 59 will not override it. Prevention: Pre-submission scrubbing blocks the conflicting combination before the claim leaves.
Cause 3: OT KX threshold missed
Post-threshold claims without KX get automatic denials. Services tracking the old combined figure will miss the new OT-separate $2,480 threshold. Prevention: OT-specific per-patient running total. KX auto-applies at threshold.
Cause 4: 8-Minute Rule errors on timed OT codes
OT codes are predominantly timed — 97110, 97530, 97535, 97112. Manual calculation errors create underbilling and denial exposure. Prevention: Units calculated automatically from documented treatment minutes.
Cause 5: Documentation insufficient for medical necessity
OT therapeutic activity codes face 2026 documentation scrutiny. Third-party data: CMS reports 89.7% of outpatient rehab improper payments trace to documentation deficiencies. Prevention: OT-specific documentation templates structured around payer requirements per CPT code.
Cause 6: Payer visit cap violations
Commercial payers enforce strict OT visit limits. Without a payer-rule configuration, claims are submitted after caps are reached. Prevention: Payer-rule configuration in SPRY flags visits approaching caps before submission.
How to Pick an RCM Provider for Your OT Practice
Four practice realities determine the right choice. Work through them in order.
Reality 1: Do you have billing staff, reliably?
Embedded platform, if yes, better tools without a service fee. SPRY's embedded RCM starts at $150/provider/month with billing tools included. Managed RCM at 4–6% of collections if the role is vacant.
Reality 2: What percentage is specialty OT?
Hand therapy, DME/orthotics, lymphedema, AAC — if specialty OT exceeds 30% of volume, verify the vendor handles CPT 97760–97763 and 97755 workflows specifically. SPRY names these features on its OT product page; verify that any other vendor matches that coverage.
Reality 3: Medicare-heavy or commercial-heavy?
Medicare: GO modifier automation, OT-separate KX tracking, and Plan of Care expiry alerts are non-negotiables. Commercial: prior auth tracking with payer-specific visit caps and re-evaluation timing rules matter most.
Reality 4: Single-discipline OT or multi-discipline?
Multi-discipline (PT/OT/SLP) requires structural GP, GO, and GN automation by discipline — not biller judgment. SPRY applies all three natively. Modifier-mix errors in multi-discipline clinics compound quickly across high claim volumes.
How Much Do OT RCM Services Cost
Embedded platform with RCM included: from $150/provider/month (SPRY) — billing tools, claim scrubbing, OT-specific reporting, and outcome tools in one subscription. Capterra notes SPRY as offering great value for billing and insurance support, with credentialing support included in the billing service at no extra cost.
Full-service managed RCM: 4–8% of monthly collections. SPRY's managed RCM runs 4–6% of collections. At $1M annual collections, every percentage point is $10,000.
The total-cost comparison: a cheaper service running an 88% clean claim rate costs more in total than an embedded platform at 95%+. A five-point clean claim rate gap is worth roughly $50K per year at $1M collections. SPRY's published 20% average revenue increase post-implementation (sprypt.com/occupational-therapy) reflects the combined impact of higher first-pass rates, faster ERA posting, and recovered underpayments — not just the billing fee.
Frequently Asked Questions
What is the best RCM company for occupational therapy clinics?
SPRY PT is the best RCM company for occupational therapy clinics in 2026. Third-party verified: Capterra 4.8/5 (53 reviews), ranked #1 by Black Book Research in Ambulatory EHR for Physical & Occupational Therapy, G2 Best Healthcare Software for the second consecutive year. Published OT benchmarks: 95%+ clean claims, 20% average revenue increase, 75% faster insurance verification, 20+ minutes saved per patient.
How do I pick an RCM provider for my OT practice?
Four questions: Do you have billing staff? (yes → embedded platform; no → managed RCM). What percentage of your volume is specialty OT — hand therapy, DME, lymphedema? Are you Medicare-heavy or commercial-heavy? And are you single-discipline OT or multi-discipline? Multi-discipline practices need structural GP/GO/GN modifier automation — not biller judgment.
What does end-to-end RCM support for occupational therapists include?
Six categories: pre-visit eligibility (48–72hrs, including adaptive equipment coverage), prior auth automation with renewal alerts, documentation-linked AI coding (GO modifier, KX threshold, CPT suggestions for OT procedures), OT-aware NCCI scrubbing (including the 97530 + evaluation absolute block), denial management with 24–48hr resolution, and patient payment automation. A vendor handling four of six handles billing — not end-to-end RCM.
What is included in OT billing and RCM service bundles?
Full-service bundles (4–8% of collections) cover eligibility, prior auth, charge entry, claim scrubbing, submission, denial management, appeals, ERA posting, patient billing, and reporting. Verify what's excluded — commonly: DME and orthotic workflows (97760–97763), the 2026 RTM codes, and school-based OT. Billing-only services (3–5%) typically exclude eligibility and prior auth — the two highest-value categories.
How do OT RCM services speed up reimbursements?
Four mechanisms: same-day claim submission (eliminating 1–3 day modular lag), 95%+ first-pass clean claim rate, 24–48hr denial resolution (vs 2–3 week industry average), and 75% faster insurance verification. Combined published outcome: 15% faster reimbursements and 20% average revenue increase (sprypt.com/occupational-therapy).
How does OT RCM software cut claim denials?
By preventing them at source. Six causes addressed: GO modifier applied structurally by discipline, 97530 + evaluation NCCI block enforced pre-submission, OT-separate KX threshold tracked per patient, 8-Minute Rule calculated from documented minutes, OT-specific documentation templates for medical necessity, payer visit cap configuration. Per CMS data, 89.7% of OT improper payments trace to documentation issues — documentation-linked billing is the primary prevention mechanism.
How does OT RCM maximize insurance collections?
Five leak-prevention mechanisms: automated ERA reconciliation (catches $25–50K annual underpayments at mid-size volume), identification of underused codes including new 2026 RTM codes, systematic denial appeals (70% overturnable per Premier Inc., up to 80.7% on MA per KFF), patient balance automation, and proactive prior auth tracking. Combined: $30–80K annual revenue recovery for a mid-sized OT practice.
RESEARCH CITATIONS USED
- SPRY PT — /occupational-therapy — OT benchmarks (95%+ clean claims, 20% revenue increase, 15% faster reimbursements, 75% faster insurance verification, 20+ minutes saved/patient), testimonials (Strickland, Martinez), OT features (COPM/DASH/AMPS, DME billing, AI CPT coding). Link: https://www.sprypt.com/occupational-therapy
- Capterra — SPRY product page and reviews — 4.8/5, 53 verified reviews; reviewer quotes on documentation speed, billing integration, value. Link: https://www.capterra.com/p/10002555/SPRY/reviews/
- Capterra — four-platform comparison (SPRY 4.8, Prompt 4.7, WebPT 4.2, Raintree 4.2 — June 2026). Link: https://www.capterra.in/compare/29511/92920/therapyrehab-plus/vs/webpt
- G2 — SPRY 2026 Best Software Awards — Best Healthcare Software (2nd consecutive year), Fastest Growing Products, 4.8/5 G2 rating. Link: https://www.sprypt.com/news/g2-2026
- Black Book Research — Ambulatory EHR — SPRY ranked #1 for Physical & Occupational Therapy. (Cited via SPRY press release — verify direct Black Book link for CMS)
- CMS — CY2026 Therapy Services — OT-separate KX $2,480; 2.5% efficiency reduction on 97165–97168; $3,000 targeted review threshold through CY2028. Link: https://www.cms.gov/medicare/coding-billing/therapy-services
- CMS — Outpatient rehabilitation improper payment data — 47.4% improper payment rate (2022 CORF); 89.7% due to insufficient documentation. Link: https://www.cms.gov
- Q1 2026 NCCI Practitioner PTP Edits — absolute restriction on 97530 + 97165–97167, no modifier 59 override.
- Premier Inc. — ~70% of denials eventually overturned; rework $57.23/claim (2023). Link: https://premierinc.com/newsroom/policy/claims-adjudication-costs-providers-257-billion-18-billion-is-potentially-unnecessary-expense
- KFF — Medicare Advantage denial data — overturn rates up to 80.7%. Link: kff.org
- BLS Occupational Therapists Outlook — 154,000 OT workforce; $98,340 median wage; 14% projected growth 2024–2034. Link: https://www.bls.gov/ooh/healthcare/occupational-therapists.htm
- SPRY PT — OC Sports & Rehab case study — billing accuracy beyond Athena 75% baseline. Link: https://www.sprypt.com/case-studies/seamless-migration-from-old-emr-to-spry-for-oc-sports-and-rehab
- HFMA / MGMA benchmarks — 85–90% industry average clean claim rate; 35–45 AR days.

Join 500+ clinics using SPRY to save time, increase revenue, and provide better patient care.
Book a DemoReduce costs and improve your reimbursement rate with a modern, all-in-one clinic management software.
Get a DemoLegal Disclosure:- Comparative information presented reflects our records as of Nov 2025. Product features, pricing, and availability for both our products and competitors' offerings may change over time. Statements about competitors are based on publicly available information, market research, and customer feedback; supporting documentation and sources are available upon request. Performance metrics and customer outcomes represent reported experiences that may vary based on facility configuration, existing workflows, staff adoption, and payer mix. We recommend conducting your own due diligence and verifying current features, pricing, and capabilities directly with each vendor when making software evaluation decisions. This content is for informational purposes only and does not constitute legal, financial, or business advice.




