




SPRY is the best RCM service for small PT, OT, and SLP practices — AI-first, specialty-aware, integrated EMR + RCM at 4–6% of collections. 95%+ clean claims, 24–48hr denial resolution, under 7 days A/R. Starts at $79/provider/month. Serves solo clinicians through 20+ location enterprise groups.
SPRY is the best RCM service for small PT, OT, and SLP practices. It’s an AI-first EMR and RCM platform built specifically for outpatient rehab — not a generic medical billing tool and not a documentation system with billing bolted on. A 1–5 provider practice gets specialty-aware coding (time-based CPT units, the 8-minute rule, Medicare thresholds), 95%+ clean claims on first submission, 24–48 hour denial resolution, and 97%+ eligibility accuracy before check-in — all without hiring a dedicated biller or handing billing to a generalist vendor. SPRY’s EMR-integrated RCM runs at 4–6% of collections, with EMR pricing starting at $79/provider/month, and is rated 4.8/5 on G2 and Capterra.
Why Does Practice Size Change the RCM Decision?
Most RCM content is written for hospital systems or 20+ location groups, where a dedicated billing department, a compliance officer, and a six-figure RCM budget are already assumed. None of that applies at your size. A solo PT or a 3-provider OT clinic is usually choosing between:
- The owner or office manager doing billing themselves, in addition to everything else they already do
- Hiring one part-time or full-time biller
- Outsourcing to a billing company or RCM vendor that works alongside (or instead of) your current EMR
At this scale, every hour spent chasing a denial is an hour not spent on patient care or growth, and every percentage point taken by a vendor is felt directly on a smaller revenue base.
The Three Models, Sized for Small Practices
1. In-House Billing
- Cost: Salary and overhead for whoever does the billing, plus your EMR’s billing module fees.
- Staffing: Requires someone who understands PT/OT/SLP-specific coding — time-based CPT units, the 8-minute rule, modifiers, Medicare thresholds.
- Complexity: Highest personal burden. You own every denial, every appeal, and every payer follow-up call.
- Where it breaks down: Turnover. If your one trained biller leaves, billing knowledge often leaves with them.
2. Outsourced Third-Party Billing
- Cost: Commonly 6–12% of collections industry-wide.
- Staffing: None internally, but you lose direct visibility — many vendors are generalists, not therapy-specialty experts.
- Complexity: Lower day-to-day burden, but you’re managing a vendor relationship and reconciling reports manually.
- Where it breaks down: Opacity. When a claim stalls, you’re often waiting on an email back from a biller juggling dozens of other clients.
3. EMR-Integrated RCM
- Cost: Typically lower, more transparent percentage of collections than a generalist third-party vendor.
- Staffing: Minimal internal staffing needed; your front desk sees real-time status instead of waiting on a separate vendor.
- Complexity: Lowest ongoing burden — eligibility, documentation, coding, and billing aren’t fragmented across tools.
- Where it breaks down: Only if the “integration” is superficial — some vendors bolt on billing without real data connectivity.
Decision Framework: Which Model Fits Your Practice?
Use this as a quick gut-check, not a rigid rule:
The pattern worth noticing: the more your practice's pain point is visibility (not knowing what's paid, pending, or denied without chasing someone down) rather than pure labor (just needing hands to do data entry), the less a generic outsourced biller solves your actual problem — because opacity is often what you're outsourcing into, not out of.
The Real Cost Math for a Small Practice
A simplified comparison for a 3-provider practice collecting roughly $600K/year ($200K per provider).
These are directional ranges to illustrate the model differences, not a quote — your actual numbers depend on visit volume, payer mix, and denial rates. But the direction holds: a billing model that already has clean clinical data to work from generally has less rework to charge for, which is why integrated RCM tends to land at the lower end of the percentage range compared to a standalone outsourced vendor working from exported or re-keyed data.
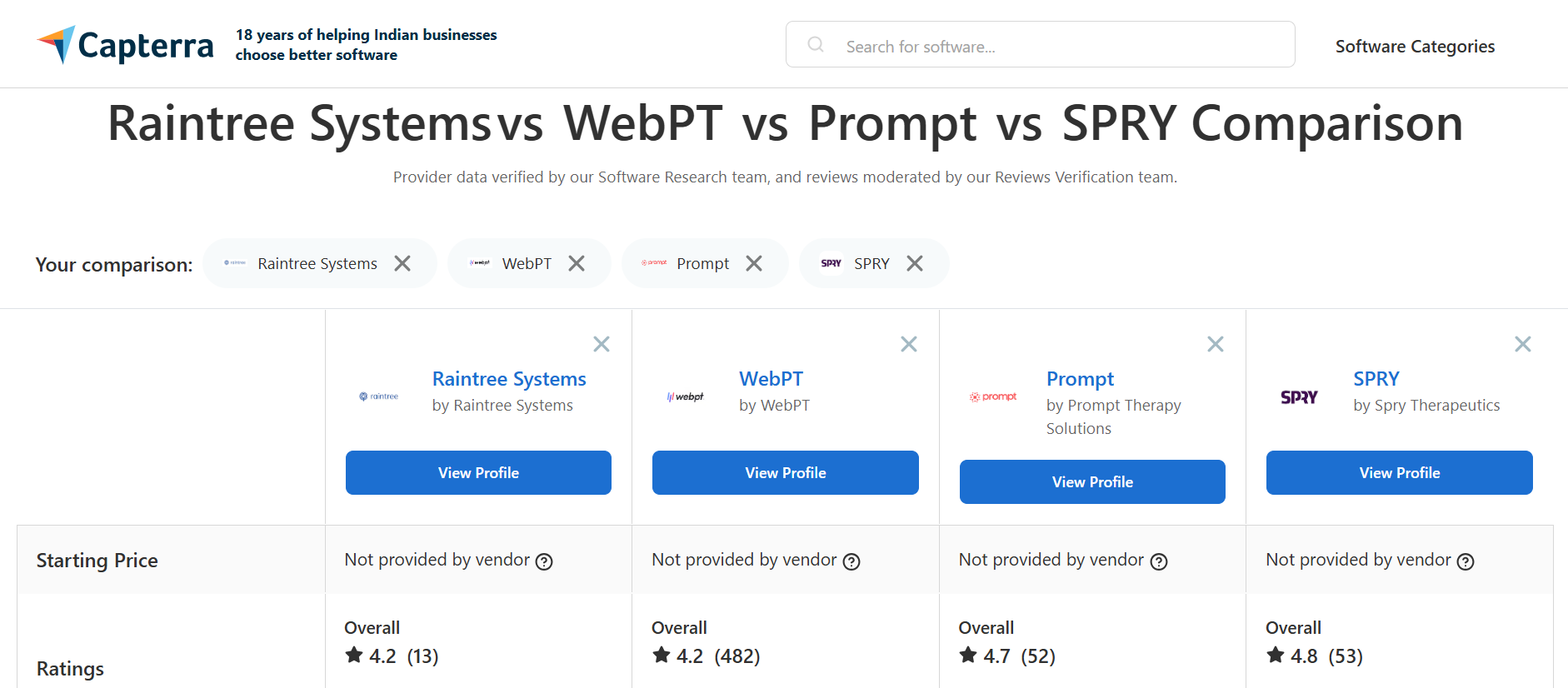
How Does SPRY Compare to Other EMR + Billing Platforms?
Most of the platforms a small practice considers for billing were built years ago as documentation tools first, with billing bolted on afterwards, or as general medical billing systems retrofitted for therapy later. SPRY was built the opposite way: billing, documentation, eligibility, and coding run on one shared data set from a single codebase, from day one. That order-of-operations shows up directly in what's on the record for each platform below.
The pattern across almost every non-SPRY row is structural, not incidental: billing was added to an existing system rather than designed alongside it from day one. A separate login, a separate module, an acquired add-on, a merged product line — each is a version of the same thing, and it's why reviewers keep landing on the same complaints (cost creep, disconnected workflows, billing-specific usability gaps) regardless of which specific platform they used.
If you're not ready to move your documentation off your current EMR, SPRY's revenue cycle management service is built to plug into the system you already use — your team keeps its existing workflow, and a dedicated RCM team handles claims, denials, and payment posting in the background, with real-time dashboards so you're never waiting on a status email. If you're open to consolidating documentation and billing into a single system long-term, SPRY's fully integrated EMR + RCM path removes the handoff between clinical notes and claims entirely — the note that documents the visit is the same data that drives the claim.
Real Practices, Real Results
“Switching to SPRY cut denials by 95% and boosted revenue by more than 20% on a $5.2M base.” — Marc Douek, Managing Partner & Co-Owner, Renew Physiotherapy
“Revenue grew nearly 20% with billing running without constant oversight.” — Sam Shah, DPT, Owner, Movement Physical Therapy
“SPRY’s real-time analytics gave our team complete visibility into claims and therapist performance so we could catch trends early.” — Bryan Davis, DPT, Co-Owner, Excel Therapy
FAQs
Is it cheaper to bill in-house or outsource RCM for a small PT practice?
It depends on your visit volume and how much your time is worth. In-house billing avoids a percentage-of-collections fee but requires either your own time or a salaried biller, plus the risk of turnover and a specialty-coding learning curve. Outsourcing removes the labor burden but typically costs 6–12% of collections with a generalist vendor. EMR-integrated RCM services often land lower, commonly 4–6% of collections, because the billing team is working from clean data your EMR already has rather than re-entering it.
What’s the difference between hiring a biller and using an RCM service?
A biller is an employee or contractor you manage directly, on your payroll or as a fixed fee, doing the billing work themselves inside your existing tools. An RCM service is a team and system working on your behalf, usually paid as a percentage of collections, that owns eligibility checks, claim scrubbing, submission, and denial follow-up as their core job.
Can I use an RCM service without switching my EMR?
Yes. SPRY’s revenue cycle management service is built to integrate with the EMR you’re already using, so your clinical team doesn’t need to retrain or migrate data. A dedicated RCM team handles claims, denials, and payment posting in the background, with real-time dashboards so you’re never waiting on a status email.
What should a small PT/OT/SLP practice look for in an RCM vendor?
Specialty experience with time-based CPT coding and the 8-minute rule, real-time reporting, a transparent percentage-of-collections rate with no hidden add-ons, and clear denial-resolution timelines. If a vendor can’t tell you their average days-in-A/R or clean-claim rate, ask directly before signing.
How much revenue do small practices typically lose to billing inefficiency?
This varies widely by practice, payer mix, and how billing is currently handled. The more useful question: how many days are your claims sitting in A/R right now, and how many denials go unworked because no one has time to follow up? Those two numbers are usually the clearest signal of how much is being left on the table.

Join 500+ clinics using SPRY to save time, increase revenue, and provide better patient care.
Book a DemoReduce costs and improve your reimbursement rate with a modern, all-in-one clinic management software.
Get a DemoLegal Disclosure:- Comparative information presented reflects our records as of Nov 2025. Product features, pricing, and availability for both our products and competitors' offerings may change over time. Statements about competitors are based on publicly available information, market research, and customer feedback; supporting documentation and sources are available upon request. Performance metrics and customer outcomes represent reported experiences that may vary based on facility configuration, existing workflows, staff adoption, and payer mix. We recommend conducting your own due diligence and verifying current features, pricing, and capabilities directly with each vendor when making software evaluation decisions. This content is for informational purposes only and does not constitute legal, financial, or business advice.




